Rajesh N. Keswani , MD and John E. Pandolfino, MD, FACG, of the Division of Gastroenterology, Feinberg School of Medicine, Northwestern University , Chicago, share insight from their research published online early in the Red Journal.

ACG: Explain the genesis of your research and what prompted this study.
Dr. Pandolfino: Quality is a top priority in the endoscopy lab and we wanted to ensure that all patients at Northwestern receive high-level care that is standardized across the entire practice. Given the fact that adenoma detection rate has surfaced as a clear quality metric, this was an appropriate first step in our comprehensive program to guarantee quality across all aspects of digestive disease management.
ACG: Explain the significance of your findings and
relationship between physician report cards and the implementation of institutional standards with improved screening colonoscopy quality. Why do these tactics make such a difference?

Dr. Keswani: Our findings highlight that physicians need to receive data on their performance in order to focus their individual quality improvement efforts. In the absence of a “report card”, it is difficult for physicians to understand which areas of their clinical practice require improvement. Of equal importance, our findings stress the critical importance that medical leadership can have in quality improvement. By simply setting expectations that all physicians practice at a high practice level, the quality of colonoscopy for all endoscopists is markedly improved.
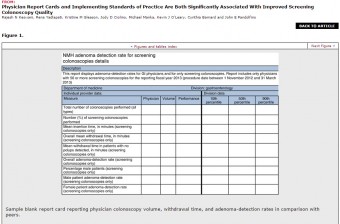
ACG: Is the Physician Report Card digital or print?
Dr. Keswani: The physician report card is delivered by paper, but a digital version is shown in Figure 1.
ACG: Can this report card tie in at all with GIQuIC? If so, how?
The report card we distributed is similar to GIQuIC in that it provides physicians the ability to benchmark their performance to peers; a unique benefit to GIQuIC, however, is the ability to additionally benchmark to peers outside their individual institution, which may be vital for small practices. However, in contrast to GIQuIC, using an institutional data warehouse as we did in this study, allows for adenoma detection rates to be automatically calculated. For large institutions which perform thousands of screening colonoscopies annually, this automated data collection markedly reduces the burdens associated with calculation of adenoma detection rates.
ACG: What do patients need to know?
Dr. Pandolfino: Patients should expect high-quality care and it is the responsibility of the leadership to ensure that the staff has the appropriate feedback and instruction to attain these high-levels.
ACG: How can endoscopy labs best (efficiently) implement PRC and SOPs? Are both required or can one be implemented without the other? Are there models or best practices that are available to use? Any tips for implementation?
Dr. Keswani: I think the first important take home message is that all endoscopy labs should be regularly calculating adenoma detection rates and distributing the results to physicians and either benchmark to other physicians in the practice or nationally. While there are many ways to calculate adenoma detection rates, I would advise gastroenterologists to interface with their endoscopy center or hospital quality leadership and institutional informatics specialists to streamline the process as much as possible. For our institution, utilizing a data warehouse that aggregates endoscopy reports, billing, and a pathology database allowed for this process to be feasible in a large endoscopy practice.
Standards of practice are not and should not be unique to colonoscopy but I would urge that a focus be maintained on outcomes (such as adenoma detection rates) rather than what are called process measures (such as withdrawal time); process measures may be easier to measure but are not strictly associated with clinical outcomes and may receive more resistance from physicians. Establishment of standards of practice should occur in a multidisciplinary group of administration, physicians, and nurses. While both report cards and standards of practice are not required, we have shown that they are complementary and would urge physicians to consider utilizing them in conjunction.
ACG: Any final thoughts?
Dr. Keswani: While this study was conducted for screening colonoscopy, the concepts are not unique to even gastroenterology. Physicians share a common desire to treat patients to their best ability. Providing feedback and guidance can help us all achieve that desire
About the Authors
John E. Pandolfino, MD,FACG, is chief of the division of gastroenterology and hepatology at Northwestern Memorial Hospital, and senior author of the article
Rajesh N. Keswani, MD, is an interventional gastroenterologist with Northwestern Medicine, and is lead author of the article.
Access the full article, “Physician Report Cards and Implementing Standards of Practice Are Both Significantly Associated With Improved Screening Colonoscopy Quality,” in the Advanced Online Publication (April 14, 2015) section of The American Journal of Gastroenterology website.