A longstanding priority for American College of Gastroenterology is to educate the public and physicians about the remarkable effectiveness and safety of colonoscopy in the hands of trained and skilled endoscopists. PowerPoint slides for physicians, patient education materials including a video, and the ACG CRC Screening Guidelines are among the resources for physicians.

Colorectal Cancer (CRC) Community Education Toolkit
The ACG’s ongoing commitment to colorectal cancer awareness includes helping physicians educate their patients and communities about the importance of screening. These CRC awareness efforts are highlighted every year during March Colorectal Cancer Awareness Month and include a CRC Community Education Toolkit containing a wealth of resources, key messages, tips, and downloadable materials.
Available Colorectal Cancer (CRC) Awareness Graphics
ACG has developed a range of graphics, including two powerful and informative infographics, to help in your colorectal cancer awareness efforts. The College encourages you to print and share these with your patients, on your website, in your office, and via social media channels such as Twitter and Facebook. Explore more downloadable graphics.

Highlights of March CRC Month Community Outreach

ACG Colorectal Cancer Screening Guidelines
The American College of Gastroenterology has issued updated screening guidelines for colorectal cancer in the March issue of The American Journal of Gastroenterology. The guidelines offer new graded recommendations for screening in an update of those published by ACG in 2009. The co-authors are Aasma Shaukat, MD, MPH, FACG; Charles J. Kahi, MD, MSc, FACG; Carol A. Burke, MD, FACG; Linda Rabeneck, MD, MPH, MACG, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist); and Douglas K. Rex, MD, MACG. Click here to read the guidelines.
Changes in the 2021 ACG Clinical Guidelines on Colorectal Cancer Screening from the 2009 ACG Recommendations (Appendix 2)
- Age to initiate CRC screening in average risk men and women is lowered to 45
- Decision to offer CRC screening beyond age 75 should be Individualized
- African Americans should start screening at age 45, but special efforts are required to improve screening rates and reduce disparities in treatment and outcomes
- Colon capsule is added as an option for CRC screening for individuals unwilling or unable to undergo colonoscopy or a FIT. If negative screening may be repeated in 5 years
- Suggestion to initiate CRC screening at age 40 or 10 years before the youngest affected relative, then resume average-risk screening recommendations for individuals with CRC or advanced polyp in one FDR at age ≥ 60. Colonoscopy or FIT are reasonable options
- Endoscopist should measure quality indicators for screening colonoscopy and achieve minimum benchmarks for cecal intubation (>=95%), adenoma detection rate (>=25%) and withdrawal time (>=6 minutes)
- Suggestion to use low dose aspirin, in addition to CRC screening, in individuals between the ages of 50-69 with a cardiovascular disease risk of >10% over the next 10 years, who are not an increased risk for bleeding and willing to take aspirin for at least 10 years to reduce the risk of CRC
- Organized screening programs should be developed to improve adherence to CRC screening and follow-up of a two-stage screening test if positive
- The following strategies may be implemented to improve organized screening: Patient navigation, patient reminders, clinician interventions, provider recommendations and clinical decision support tools
- A positive multitarget stool DNA test followed by a colonoscopy with no findings should not prompt any further work up, and repeat screening should be offered at 10 years
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer.
Patients at average risk of colorectal cancer who have a clean colonoscopy do not need to repeat the test for 10 years. This and many other practical recommendations for cancer prevention were issued in “Guidelines for Colonoscopy Surveillance After Screening and Polypectomy,” a consensus update issued by the U.S. Multisociety Task Force on Colorectal Cancer. Click here to read the guidelines.
Slides for Physicians Developed by ACG Experts
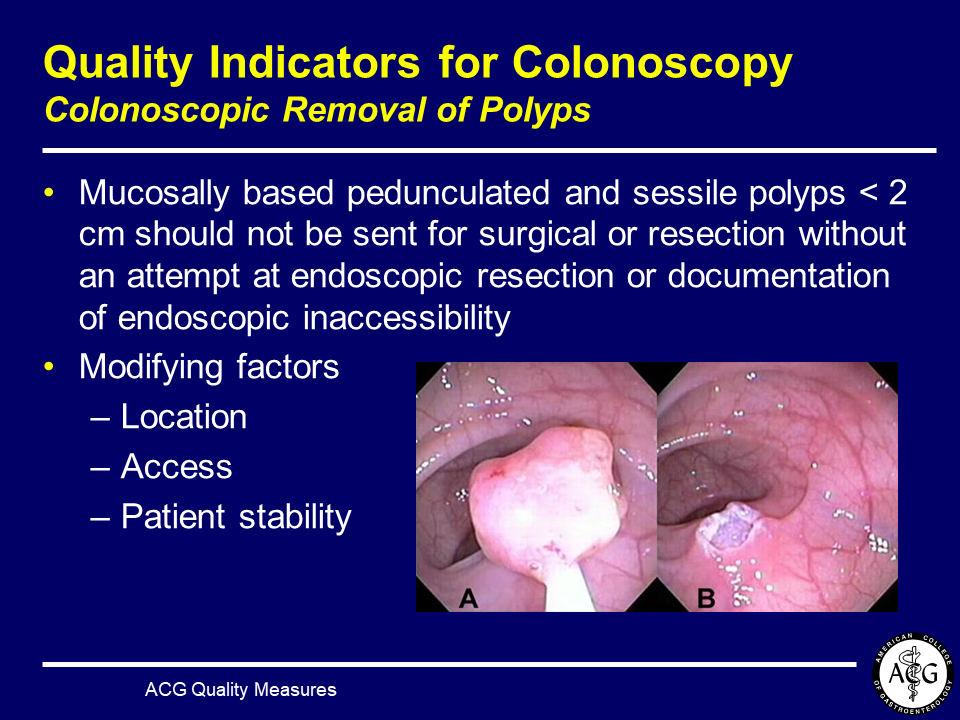
Quality Measures for Colonoscopy – One of the ACG’s primary objectives is to focus attention on the importance of quality colonoscopy. The overall impact of colonoscopy depends critically on high quality baseline examinations. Therefore, ACG recommends that screening colonoscopies be performed by appropriately trained and skilled examiners who are dedicated to consistent performance of high quality examinations. The American College of Gastroenterology has both endorsed and developed quality indicators for colonoscopy. ACG’s Subcommittee on Colorectal Cancer Screening and Surveillance developed a slide set for physician education reviewing quality measures for colonoscopy to educate endoscopists and enhance the effectiveness of colonoscopy in cancer detection. Developed by distinguished experts, the new slides offer ACG member physicians a convenient overview of key quality issues such as:
- Quality – why should you care?
- Published quality indicators for colonoscopy
- Standards for documentation of endoscopic procedures
Slide Set: Understanding Colorectal Cancer for the Patient Audience Updated 2021

Slide Set: Quality and Efficiency Measures for the Colonoscopy
Patient Brochure & Flyer
Created by the ACG Public Relations Committee, these new patient education tools include evidence-based recommendations from the 2021 update to ACG’s Clinical Guidelines on Colorectal Cancer Screening (Shaukat, et al.) and highlight the importance of colorectal cancer screening starting at age 45 for average risk adults. These materials present a clear, concise overview of colorectal cancer risk factors and screening strategies.
Patient Tri-Fold Pamphlet

45 is the New 50!
“45 is the New 50! You Can Prevent Colorectal Cancer” empowers patients to take action against colorectal cancer. Covering recommendations from the American College of Gastroenterology, this brochures conveys the safety and importance of colorectal cancer screening starting at age 45 for average risk individuals.
Flyer

Colorectal Cancer: You Can Prevent It
This flyer for ACG members reflects the College’s commitment to educating the public about the lifesaving potential of colorectal cancer screening. Using evidence-based recommendations from the 2021 ACG Clinical Guidelines on Colorectal Cancer Screening (Shaukat, et al.)