Medicare physician reimbursement reform has been a longstanding policy priority for ACG, and after years of incremental fixes and stopgap solutions, Congress is finally taking a closer look. Recent activity on Capitol Hill reflects a growing recognition from both parties that the current system is broken, and ACG is helping shape the path forward.
ACG members: H.R. 8163 was just passed out of a key House committee and would update a decades-old budget neutrality requirement — bringing stability to the reimbursement system. Call your Representative today and urge them to co-sponsor!
ACG Engages the GOP and Democratic Doctors Caucuses
As Congress deliberates over federal spending bills and other legislation, the physician members of Congress that make up the GOP and Democratic Doctors Caucuses jointly released a Medicare reimbursement reform draft proposal. This draft outlines a framework for meaningful reform, like incorporating inflation-based updates tied to the Medicare economic index (MEI), modernizing the decades-old budget neutrality requirement, updating practice expense (PE) calculations, and improvements to the Medicare fee for service quality reporting program (MIPS).
ACG’s response made clear that the status quo is simply unsustainable, emphasizing:
- Declining Medicare physician reimbursement impacts patient care and access to health care services. Recent policy changes from CMS, like the efficiency adjustment and facility PE cuts, have only exacerbated the situation.
- The “budget neutrality” provision, unchanged since 1992, is unfair, unwarranted, and is a leading cause of annual legislative emergencies.
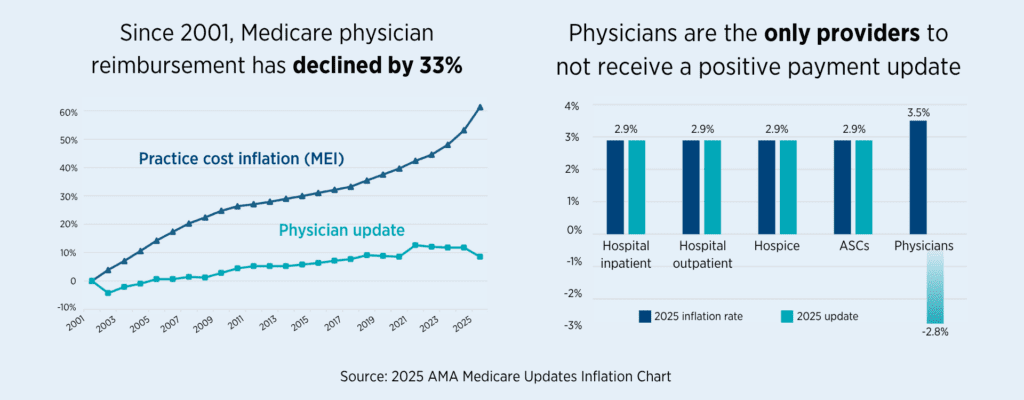
- Unlike hospitals and facilities, the Medicare physician fee schedule lacks an annual inflation adjustment, contributing to practice consolidation, provider burnout, especially among smaller independent and rural practices.
- The federal government exempts small businesses with fewer than 50 employees from various employment and labor laws. Congress should follow the same precedent and exempt small and independent practices, or those in professional shortage areas, from costly and burdensome regulatory/reporting requirements.
The Growing Gap Between What Care Costs and What Medicare Pays
GI practices are facing rising practice costs (made worse by healthcare workforce shortages) as well as increasing medical device and equipment prices. Yet, reimbursement rates continue to decrease.
Since 2019, the MEI has increased by 24%. Meanwhile, in the same period, Medicare reimbursement for diagnostic colonoscopy (CPT 45378) has decreased by a total of 15 percent. That widening gap between Medicare payments and the cost to provide care is felt most acutely by practices in rural and underserved areas.
A more comprehensive MEI update would help to ensure independent practices can continue to serve their patients.
ACG Shares Testimony with Key House Committee
On May 20th, the U.S. House Energy and Commerce Health Subcommittee held a hearing entitled, “Examining the Medicare Physician Fee Schedule, MACRA, and Opportunities for Payment Reforms.”
Top highlights from the hearing
Rep. John Joyce, MD (R-PA): “Raise your hand if you agree with the statement: Having more physicians in independent practice generally reduces cost system-wide and empowers the doctors to spend more time directly with the patient”
All Witnesses: *Raise hands*
Ahead of the hearing, ACG submitted formal testimony, which echoed our themes from the Doctors Caucus draft and incorporated evidence on the true administrative burden of MIPS compliance.
For example, in the annual Medicare payment regulations, CMS estimated roughly 38 hours of work per clinician was required for MIPS participation, at a cost of nearly $7,800. However, available research suggests those figures are woefully low. One qualitative study revealed that physician practices across the U.S. spent more than 200 hours per physician on MIPS-related activities, at an average cost of $12,811.
Also, over 50% of all Medicare patients are enrolled in Medicare Advantage plans. There is no reason why physician practices must devote limited resources to participate in two separate Medicare quality reporting programs (MIPS/MACRA and Medicare Advantage). Congress should align and combine these two programs to ease practice management challenges and unnecessary burdens.
We need policies that are rooted in reality and reflect the true burdens borne by physician practices.
A Bipartisan Step Forward—But Still a Ways to Go
Last week, the U.S. House Committee on Ways & Means debated various bills, including the Provider Reimbursement Stability Act of 2026 (H.R. 8163), introduced by Rep. Greg Murphy, MD (R-NC). Remarkably, the bill passed with unanimous support, a genuinely rare bipartisan feat in today’s Congress.
The bill addresses a crucial structural problem in the Medicare physician payment system: the budget neutrality threshold, which has stood at $20 million since it was set more than thirty years ago. Under current law, any increase to one specialty’s reimbursement triggers automatic cuts to another, a ‘robbing Peter to pay Paul’ paradox that limits meaningful reforms. H.R. 8163 would raise the antiquated budget neutrality threshold to $54 million, while limiting the volatility of year-to-year conversion factor changes.
This is a meaningful development—but we recognize it is one step in a much longer process. The bill still requires a full House vote, and there is no companion bill currently in the Senate.
ACG leaders made the case for this exact bill during our Advocacy Day in April, across more than 200 meetings with members of Congress and their staff. This progress reflects what happens when we share the perspective of clinical GI and independent practices with Congress. ACG will continue to engage as this legislation advances and keep members informed at every step.
But you don’t need to be in Washington to make a difference. Reach out to your Representative and Senators today, urge them to co-sponsor H.R. 8163, and share your own story of how Medicare reimbursement cuts are affecting your patients and your practice. Nobody will advocate for GI care if we don’t.