Optimizing Bowel Preparation for Colonoscopy: Insights from the USMSTF Recommendations
 Rachael Hagen DO1 and Joseph C. Anderson, MD, FACG1,2
Rachael Hagen DO1 and Joseph C. Anderson, MD, FACG1,2

1University of Connecticut School of Medicine, Farmington, CT
2VA Medical Center, White River Junction, VT; Geisel School of Medicine at Dartmouth, Hanover, NH.
This summary reviews Jacobson BC, Anderson JC, Burke CA, et al. Optimizing Bowel Preparation Quality for Colonoscopy: Consensus Recommendations by the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol. 2025;120(4):738-64.
Read the article in The American Journal of Gastroenterology
Correspondence to Joseph C. Anderson, MD, FACG, Co-Editor-in-Chief. Email: EBGI@gi.org
Keywords: bowel prep, colonoscopy; colorectal cancer screening, USMSTF
Pre-Colonoscopy. What pre-colonoscopy interventions can enhance bowel preparation adequacy? How should bowel purgatives and adjuncts be selected to optimize preparation quality?
During Colonoscopy. What techniques can improve bowel preparation quality during colonoscopy? How should bowel cleanliness be assessed and reported?
Post-Colonoscopy. What is an appropriate bowel preparation adequacy rate? What strategies should be used to manage high-risk patients for inadequate bowel preparation?
Design: A panel of content experts formulated clinical questions using the Patient, Intervention, Comparison, and Outcomes (PICO) framework. Research librarians conducted a literature review search across EMBASE, PubMed, Cochrane Reviews, and the Cochrane Central Register of Controlled Clinical Trials from January 2013 to September 2023.The United States Multi-Society Task Force (USMSTF) includes 3 representatives from each of the following societies: The American College of Gastroenterology (ACG), the American Gastroenterology Association (AGA), and the American Society for Gastrointestinal Endoscopy (ASGE). Leadership from all 3 organizations reviewed the recommendations, which were subsequently approved by each society’s governing board.As the statements were developed through expert consensus rather than the traditional guideline development process, they are designated as “Recommendations” rather than “Guidelines.” Additionally, key concepts were established based on expert consensus for topics where evidence-based recommendations could not be formulated.
Patients: Outpatients at low risk for inadequate bowel preparation.
Outcome: Improved bowel preparation quality enhances colonic mucosa visualization, facilitates precancerous lesion detection, and optimizes colorectal cancer monitoring.
Data Analysis: Recommendations were created by an expert consensus as described above. A literature review was conducted to develop recommendations. The quality of evidence supporting each recommendation was also assessed. Strong recommendations indicate that most patients should be managed accordingly and are typically associated with high or moderate-quality evidence from well-designed clinical trials and systematic reviews. In contrast, weak recommendations serve as suggestions due to limited evidence or a smaller clinical impact and are generally based on low or very low-quality evidence. When evidence-based recommendations could not be formulated, key concept statements were developed through expert consensus.
Funding: None.
Summary: Authors recommend assessing a patient’s medical history, including prior bowel preparation adequacy, to help predict preparation quality. Adherence to instructions is crucial and should be reinforced through written and verbal guidance, along with patient navigation. Dietary restrictions should be limited to the day before the procedure. Preparation regimens should be tailored to medical history, patient preference, and comorbidities, with a preference for low-volume (≤2 L) solutions to improve tolerability.1 Split-dose preparation is preferred, except for afternoon colonoscopies.
Oral simethicone is recommended to enhance visibility by reducing bubble formation, thereby improving procedural quality. The lowest effective dilution (e.g. 0.5 mL simethicone in 99.5 mL water) at a minimum dose of 320 mg should be used and administered only through an instrument channel that undergoes routinely brushing during endoscope reprocessing. The routine use of other adjuncts is not advised.
When inadequate bowel preparation is suspected, confirmation should be made by assessing preparation quality to the sigmoid colon. Bowel cleanliness should be evaluated and clearly described following endoscopist cleansing maneuvers. Endoscopists should employ strategies to enhance visualization, such as irrigation pumps, same-day rescue therapy, and the lowest effective dilution of simethicone. The term “adequate” preparation should be reserved for cases when standard surveillance intervals can be assigned based on examination findings.
Following colonoscopy, bowel preparation adequacy rates should be tracked at the level of the individual endoscopist and the endoscopy unit, with a target of at least 90%. This includes procedures cancelled for presumed inadequate preparation. Significant differences in adequacy rates may indicate deficiencies in cleansing methods during colonoscopy or inconsistencies in assessing preparation quality. When bowel preparation is insufficient for standard screening or surveillance, repeat colonoscopy should be performed within 12 months, or sooner for patients with alarm symptoms or positive non-endoscopic colorectal cancer screening tests.
For patients with a history of inadequate preparation or those at high risk, proactive interventions should be implemented to augment bowel cleansing. These may include improved patient communication, stricter dietary limitations, use of promotility agents, and methods to prevent constipation. High-risk patients should begin dietary modifications 2-3 days prior and consume 4L PEG-ELS with 15 mg of bisacodyl the afternoon before. If visualization of the ascending or transverse colon is poor but the remainder of the colonic mucosa is well visualized, the procedure should be considered equivalent to flexible sigmoidoscopy, with repeat screening recommended in 5 years or via non-endoscopic methods.
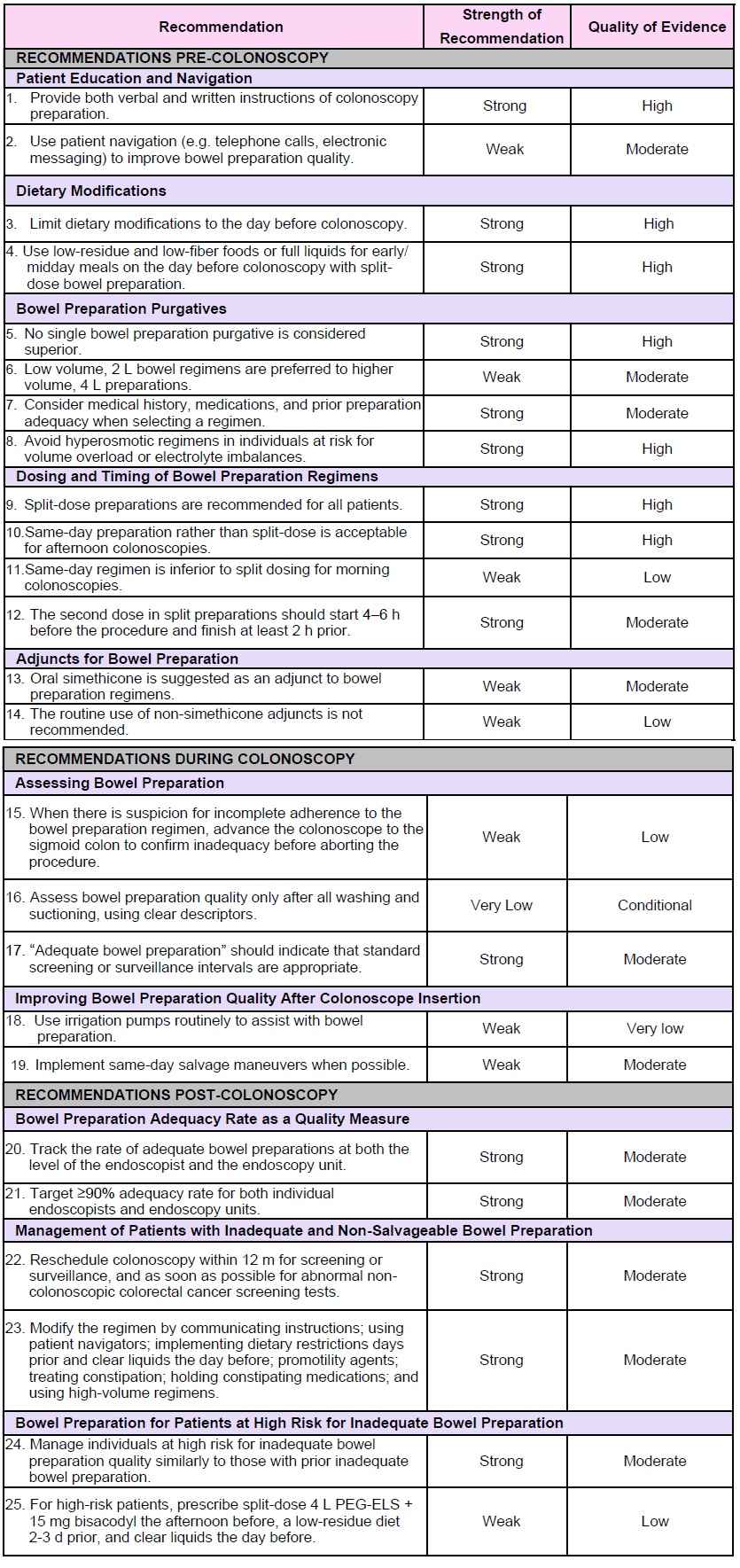
USMSTF recommendations are listed in Table 1 along with the strength of recommendation and quality of evidence.
COMMENTARY
Why Is This Important?
High-quality colonoscopy is essential for evaluation of the colon, such as detecting and monitoring precancerous lesions. Suboptimal bowel preparation decreases colonoscopy efficacy and is associated with significant adenoma and advanced adenoma miss rates.2 These recommendations update the 2014 USMSTF recommendations on optimizing bowel preparation for colonoscopy. Over the last decade, significant advancements have been made to improve bowel cleansing adequacy, patient tolerability, and procedural outcomes. In addition, many new bowel purgative options continue to emerge. Updated recommendations emphasize split-dose low-volume (≤2 L) regimens, which provide bowel preparation quality comparable to higher volume solutions while offering better tolerability. These regimens have been shown to increase adenoma and potentially sessile serrated lesion detection rates, ultimately improving the effectiveness of colorectal cancer screening and surveillance.3,4,5,6
Key Study Findings
Updated USMSTF recommendations emphasize a patient-centered approach that promoting split-dose regimens (except for patients undergoing afternoon colonoscopies) and greater flexibility in dietary modifications.
The term “adequate bowel preparation” should refer to a colonoscopy of sufficient quality to allow for the application of standard screening or surveillance intervals. A benchmark of >90% adequate bowel preparation rates is suggested for both individual endoscopists and endoscopy units to improve colonoscopy quality and detection rates. Additionally, innovations such as patient navigators, enhanced instructional methods, and artificial intelligence-driven tools have been introduced to further optimize bowel preparation quality.
Caution
The key concepts are expert panel suggestions and some recommendations are not supported by substantial evidence. They should be applied to patients on an individual basis when managing bowel preparation for colonoscopy.
My Practice
My approach for optimizing bowel preparation for colonoscopy includes prescribing low-volume, split-dose regimens to enhance patient compliance and preparation quality, reserving full-dose regimens for afternoon colonoscopies, which still demonstrate effective cleansing. To minimize ambiguity in bowel preparation assessment, I prefer standardized scoring systems with clear descriptors, such as the one used in the New Hampshire Colonoscopy Registry scale.7 Scales with clear descriptions allow for endoscopists as well as other physicians reading the note to determine whether the bowel preparation was adequate.
When inadequate bowel preparation is suspected, I confirm that the quality is inadequate by endoscopically examining the distal colon before cancelling the procedure. I also document inadequate preparation with photographs of poorly cleansed segments for improvement efforts. While salvage therapies, such as enemas, may provide additional cleansing, logistical constraints often limit reassessment.
During the colonoscopy, I perform thorough cleaning maneuvers, utilizing a vigorous water exchange approach. The use of copious water infusion in exams with residual stool can help improve the quality. I also find that removing the suction button helps to increase the rate of aspiration, making sure that I point the handle down to avoid splattering. Finally, if I snare a polyp, I will leave the snare in the biopsy channel to avoid clogging.
Bowel preparation adequacy rates are routinely tracked at our endoscopy unit to drive quality improvement. When patients present with inadequate bowel preparation despite additional cleansing efforts, we will reschedule, ideally for next-day colonoscopy. However, scheduling conflicts often preclude same-day colonoscopy completion with additional purgatives. To mitigate these issues, I proactively identify high-risk patients before their procedures, ensuring early interventions through patient navigation, enhanced communication, and reinforcement of preparation instructions. Although not preferred, for average risk patients with repeated inadequate preparation, I discuss alternative colorectal cancer screening options.
For Future Research
Future research should explore strategies to enhance bowel preparation adequacy while maintaining the improved patient tolerability of low-volume, split-dose regimens.1,8,9,10 This includes the use of novel adjuncts to optimize cleansing with smaller solution volumes. Further research is needed to evaluate the clinical impact of simethicone and its efficacy when combined with other bowel regimens. As our understanding of GLP-1 receptor agonists evolves, the approach to pre-procedure management of patient’s using these medications should be refined.
In addition, data on same-day dosing of morning colonoscopies remain limited and warrants investigation. Identifying patients at high risk for inadequate bowel preparation is essential, and artificial intelligence-based tools may play a key role in this effort. Some have already been developed to evaluate bowel preparation quality by analyzing photographs of stool before the procedure.11
Conflict of Interest
The authors have no reported conflicts of interest.
Abbreviations
ACG, American College of Gastroenterology; AGA, American Gastroenterology Association; ASGE, American Society for Gastrointestinal Endoscopy; PEG-ELS, polyethylene glycol-electrolyte lavage solution; PICO, Patient, Intervention, Comparison, and Outcomes; USMSTF, United States Multi-Society Task Force.
REFERENCES
- Oldfield EC, Johnson DA, Rex DK. Prescribing colonoscopy bowel preparations: Tips for maximizing outcomes. Am J Gastroenterol. 2023;118(5):761-764.
- Lebwohl B, Kastrinos F, Glick M, Rosenbaum AJ, Wang T, Neugut AI. The impact of suboptimal bowel preparation on adenoma miss rates and the factors associated with early repeat colonoscopy. Gastrointest Endosc. 2011;73(6):1207-1214.
- Hassan C, East J, Radaelli F, et al. Bowel preparation for colonoscopy: European Society of Gastrointestinal Endoscopy (ESGE) Guideline—Update 2019. Endoscopy. 2019;51(8):775-794.
- Jover R, Zapater P, Polanía E, et al. Modifiable endoscopic factors that influence the adenoma detection rate in colorectal cancer screening colonoscopies. Gastrointest Endosc. 2013;77(3):381-389.e1.
- Gurudu SR, Ramirez FC, Harrison ME, Leighton JA, Crowell MD. Increased adenoma detection rate with system-wide implementation of a split-dose preparation for colonoscopy. Gastrointest Endosc. 2012;76(3):603-608.e1.
- Horton N, Garber A, Hasson H, Lopez R, Burke CA. Impact of Single-_vs_Split-Dose_Low-Volume Bowel Preparations on Bowel Movement Kinetics, Patient Inconvenience, and Polyp Detection: A Prospective Trial. Am J Gastroenterol. 2016;111(9):1330-1337.
- Anderson JC, Butterly L, Robinson CM, Goodrich M, Weiss JE. Impact of fair bowel prep on adenoma and serrated polyp detection: Data from the New Hampshire Colonoscopy Registry using a standardized preparation quality rating. Gastrointest Endosc. 2014;80(3):463-470.
- Martel M, Barkun AN, Menard C, Restellini S, Kherad O, Vanasse A. Split-dose preparations are superior to day-before bowel cleansing regimens: A meta-analysis. Gastroenterology. 2015;149(1):79-88.
- Shafer LA, Walker JR, Waldman C, et al. Predictors of patient reluctance to wake early in the morning for bowel preparation for colonoscopy: A precolonoscopy survey in city-wide practice. Endoscopy International Open. 2018;6(6):E706.
- Menees SB, Kim HM, Wren P, et al. Patient compliance and suboptimal bowel preparation with split-dose bowel regimen in average-risk screening colonoscopy. Gastrointest Endosc. 2014;79(5):811-820.e3.
- Zhu Y, Zhang DF, Wu HL, et al. Improving bowel preparation for colonoscopy with a smartphone application driven by artificial intelligence. npj Digit Med. 2023;6(1):1-9.