Updated 2025 ACG Clinical Guideline for the Management of Crohn’s Disease
 Mike Z. Zhai, MD, MBA1, Rahul S. Dalal, MD, MPH2
Mike Z. Zhai, MD, MBA1, Rahul S. Dalal, MD, MPH2


1Gastroenterology Fellow, Brigham and Women’s Hospital
2Associate Gastroenterologist, Brigham and Women’s Hospital; Instructor in Medicine, Harvard Medical School
This article reviews: Lichtenstein GR, Loftus EV Jr, Isaacs KL, et al. ACG Clinical Guideline: Management of Crohn’s Disease in Adults. Am J Gastroenterol. 2025; 120(6):1225-1264.
Access the article through The American Journal of Gastroenterology
Correspondence to: Rahul S. Dalal, MD, MPH, Associate Editor. Email: rsdalal@bwh.harvard.edu
STRUCTURED ABSTRACT
Question: What are the major updates in the 2025 American College of Gastroenterology clinical guideline for the management of Crohn’s disease (CD) compared with the 2018 guideline? How do these new guidelines incorporate recent therapeutic advances and evolving evidence into clinical practice?
Design: Evidence-based clinical practice guideline using the GRADE framework, incorporating systematic literature review and consensus expert opinion.
Setting: Multicenter, multidisciplinary guideline panel convened by the American College of Gastroenterology.
Patients: Adult patients with suspected, newly diagnosed, or established Crohn’s disease, including luminal, fistulizing, and stricturing phenotypes.
Exposure or Interventions: Recommendations encompass diagnostic strategies, dietary and lifestyle interventions, corticosteroids, immunomodulators, biologics, and small molecule therapies, with special attention to new agents approved since the 2018 guidelines.
Outcomes: Induction and maintenance of clinical, endoscopic, and radiographic remission; prevention of complications; reduction in corticosteroid dependence; and patient-centered outcomes.
Data Analysis: Evidence was graded as high, moderate, low, or very low using the GRADE approach, with formulation of recommendations as strong or conditional.
Funding: American College of Gastroenterology.
Results: The 2025 updated guideline incorporates significant changes from 2018, reflecting both refinement in diagnostic approaches as well as therapeutic advances.
Diagnosis: The guidelines now provide a practical fecal calprotectin cut-off of >50-100 mg/g to distinguish inflammatory from non-inflammatory disease. It also formally endorses intestinal ultrasound (IUS) as a non-invasive, radiation-free adjunct for both diagnostic and monitoring, alongside other imaging techniques like CT or MR enterography.
Treatment: Most importantly, while mucosal healing on endoscopy remains the goal of therapy, the panel suggests against requiring patients to fail conventional therapies such as thiopurines or methotrexate before starting advanced therapies in moderate-to-severe CD, as new evidence emerged showing early intervention with advanced therapy is superior to accelerated step-up therapy.1
Mild-to-moderate CD. Mesalamine is now strongly discouraged for both induction and maintenance of luminal CD due to limited efficacy. Sulfasalazine should only be considered for patients with mild colonic CD. Budesonide at 9 mg daily remains recommended for induction in mild-to-moderate ileocecal CD but is recommended against for maintenance.
The role of dietary therapy is now recognized only in mild-to-moderate disease, citing specific data from the DINE-CD trial, which supports Mediterranean or specific carbohydrate diets in select low-risk patients with mild disease, provided close monitoring is ensured.2
Moderate-to-severe CD. Systemic corticosteroids remain induction-only agents with a strong recommendation to limit use to fewer than 3 months, and to initiate a structured taper with rapid transition to steroid-sparing regimens.
Since 2018, the therapeutic landscape has expanded considerably, and the new guidelines incorporates new IL-23 inhibitors like risankizumab, guselkumab, and mirikuzumab, as well as JAK inhibitor upadacitinib alongside established agents such as anti-TNF therapies, vedolizumab, and ustekinumab for induction and maintenance. In particular, risankizumab is preferred over ustekinumab in patients previously exposed to anti-TNF agents. New subcutaneous infliximab and vedolizumab formulations are added as new maintenance options. No specific guidance for treatment selection is provided based on the location of the disease.
Fistulizing CD. Management of fistulizing disease has also broadened. Infliximab remains first-line therapy, but adalimumab, vedolizumab, ustekinumab, and upadacitinib are now considered reasonable options for induction.
Postoperative CD. Guidelines newly recommend endoscopic monitoring at 6-12 months after surgery. It continues to support continued observation in low-risk patients, but now adds vedolizumab, in addition to infliximab, to post-operative prevention regimens in high-risk patients.
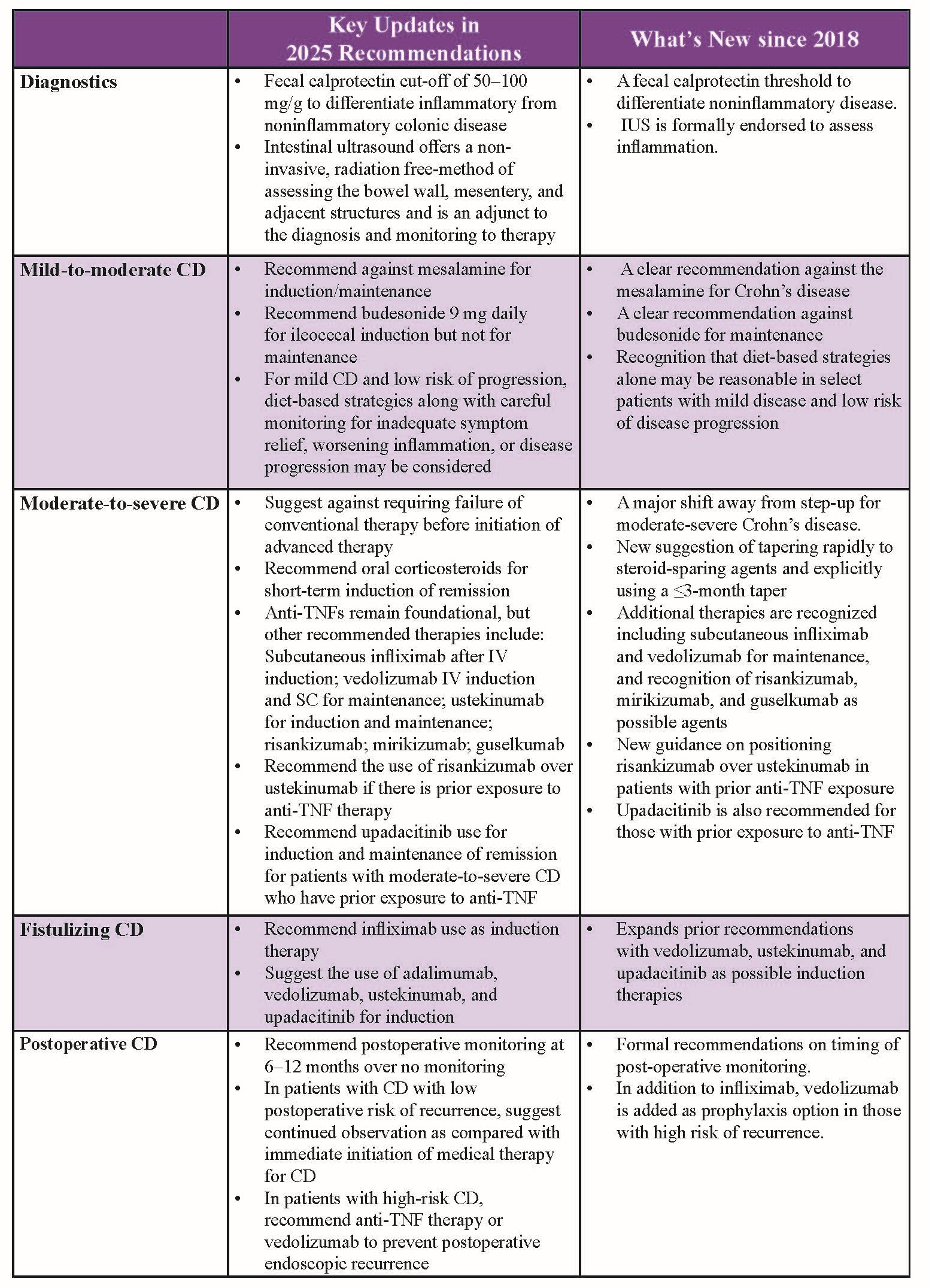
Table 1. Key Updates in Recommendations.
COMMENTARY
Why Is This Important?
Since the 2018 guideline, multiple new biologic and small molecule agents have been approved for Crohn’s disease, and data have emerged supporting earlier initiation of advanced therapies to improve long-term outcomes. The 2025 update reflects this shift toward early treat-to-target strategies, the de-implementation of ineffective agents, and individualized therapy selection based on disease phenotype, prior exposures, and patient preferences.
Key Study Findings
The update provides several practice-changing recommendations.
Caution
Despite these advances, many recommendations remain conditional and based on low-quality evidence, particularly concerning comparative positioning of agents and sequencing strategies after biologic failure. Evidence for dietary therapies also remain limited, and while they may benefit select motivated patients with low-risk disease, reliance on diet alone should not delay timely escalation in more severe phenotypes.
My Practice
In light of these updates, I will more readily consider initiating advanced therapies in treatment-naïve patients with moderate-to-severe CD, particularly those with high-risk features. Mesalamine will no longer be used in my practice for luminal disease. I will continue to be mindful of duration of corticosteroid use, and taper as soon as appropriate, with early transition to steroid-sparing maintenance therapies. With the expansion of IL-23 antagonists and upadacitinib as well as subcutaneous formulations of select advanced treatment, I will increasingly individualize treatment selection based on prior drug exposure, comorbidities, and patient preference for mode of administration.
For Future Research
Comparative effectiveness and head-to-head trials among newer biologics and small molecules are urgently needed, as are studies on sequencing strategies after treatment failure. Long-term safety data for JAK inhibitors in CD, and optimal dietary intervention protocols, are also priorities.
Conflict of Interest
The authors have no reported conflicts of interest.
REFERENCES
- Noor NM, Lee JC, Bond S, et al. A biomarker-stratified comparison of top-down versus accelerated step-up treatment strategies for patients with newly diagnosed Crohn’s disease (PROFILE): A multicentre, open-label randomised controlled trial. Lancet Gastroenterol Hepatol 2024;9(5):415–27.
- Lewis JD, Sandler RS, Brotherton C, et al. A randomized trial comparing the specific carbohydrate diet to a mediterranean diet in adults with Crohn’s disease. Gastroenterology 2021;161(3):837–52.e9.