When Is Routine Prophylactic Clipping Indicated Post-Polypectomy?

Jeffrey Lee, MD, MPH
Research Scientist and Attending Gastroenterologist, Department of
Gastroenterology, Kaiser Permanente San Francisco Medical Center, California
This article reviews Gupta S, Sidhu M, Shahidi N, et al. Effect of prophylactic endoscopic clip placement on clinically significant post-endoscopic mucosal resection bleeding in the right colon: a single-centre, randomised controlled trial. Lancet Gastroenterol Hepatol 2022; 7(2):152-160. PMID: 34801133.
Correspondence to Jeffrey Lee, MD, MPH, Associate Editor. Email: EBGI@gi.org
STRUCTURED ABSTRACT
Question: Does routine prophylactic clipping prevent clinically significant post-endoscopic mucosal resection (EMR) bleeding within the right colon for polyps > 20 mm?
Design: Randomized controlled trial.
Setting: Single tertiary medical center in Australia (Westmead Hospital, Sydney, New South Wales, Australia).
Patients: Two hundred and thirty one patients who underwent an EMR with electrocautery of non-pedunculated colorectal polyps > 20 mm were included in this trial conducted from February 2016 to December 2020; 118 were assigned to the clip group and 113 to the no clip group (control). Among the clip and control groups, the mean age of the study participants was 70 and 71 years, 41% and 50% were women, 25% and 29% were on antithrombotic agents, and mean lesion size was 35.7 mm and 37.2 mm, respectively. Antithrombotic agents were held for appropriate periods prior to colonoscopy and then re-started 48 hours after the procedure.
EMR was performed with electrocautery (ERBE ENDO CUT Q, Effect 3) after injection of succinylated gelatin (Gelofusine) mixed with 0.4% indigo carmine and 1:100,000 epinephrine. Cold avulsion and snare-tip soft coagulation were also implemented during the trial as appropriate. If deep mural injury types II-V occurred during EMR, then mechanical clip closure was performed. After EMR was completed, the endoscopist was informed about patient allocation to prophylactic clip or no-clip group.
Exposure: Prophylactic clipping (intervention) of the EMR defect vs no clipping (control). In the clip group, hemostatic clips were deployed less than 5 mm apart to close the EMR defect.
Outcome: Primary outcome was clinically significant post-EMR bleeding, defined as hematochezia necessitating emergency department presentation, hospitalization, or re-intervention within 14 days post-EMR.
Results: In the intention-to-treat analysis, clinically significant post-EMR bleeding occurred less frequently in the clip group than in the control group (4 of 118 patients [3.4%] vs 12 of 113 [10.6%]; P=0.031; absolute risk reduction 7.2% [95% CI 0.7-13.8]; number needed to treat: 13.9). (Figure 1) Clinically significant post-EMR bleeding remained lower in the clip grip versus the control group in the per-protocol analysis (1.1% vs 9.4%; P=0.019; absolute risk reduction 8.2%; number needed to treat: 12.1). There were no differences between groups in adverse events, including delayed perforation and post-EMR pain.
Funding: None
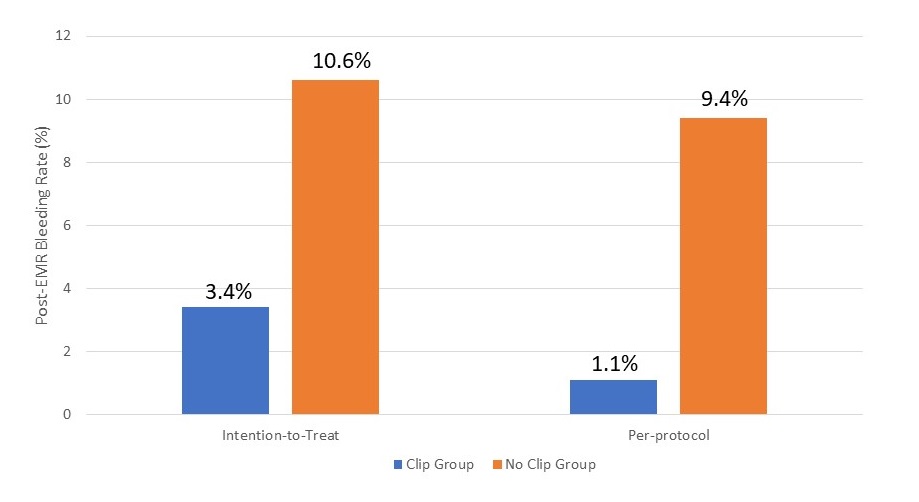
Figure 1. Post-EMR Bleeding Rates
COMMENTARY
Why Is This Important?
Despite recent advances in endoscopic resection of complex colorectal polyps, post-resection bleeding remains a problem. Clinically significant post-EMR bleeding occurs in 4%-10% of cases and is frequently seen in the right colon.1-3 Management of post-EMR bleeding can be costly and resource intensive, often requiring hospitalizations and a repeat colonoscopy. Randomized trials evaluating prophylactic clipping for prevention of post-EMR bleeding are limited and have shown discordant results in the right colon4-6. Given the conflicting evidence on this topic, this study fills an important gap by using a well-designed, randomized controlled trial to assess the impact of prophylactic clipping for the prevention of post-EMR bleeding in the right colon.
Key Study Findings
In an intention-to-treat analysis, clinically significant post-EMR bleeding in the right colon decreased from 10.6% to 3.4% with prophylactic clipping of the defect (P=0.031). In the per-protocol analysis, clinically significant post-EMR bleeding in the right colon was reduced from 9.4% to 1.1% with prophylactic clipping (P=0.019) (Figure 1). The median number of clips used was 5 across both groups. In the control group, bleeding risk was highest in the cecum (19%) compared with the risk of bleeding occurring within the rest of the right colon (3%). The benefit of clip closure was greatest for EMR defects that were 20 mm-39 mm in size and among defects located within cecum. There were no differences between groups in rates of adverse events, including perforation (<1% in each group), and in post-EMR pain (clip group, 3%; no-clip group, 5%).
Caution
The findings from this study may not be replicated in other health care settings given that this trial was conducted at a tertiary referral center with expertise in EMR. Specifically, the study endoscopists were gastroenterologists with advanced training and an established tertiary referral practice in complicated EMR.
My Practice
My general approach for placing prophylactic clips to prevent post-EMR bleeding depends on the size and location of the EMR defect, and whether the patient will need to be placed back on anticoagulants (e.g., warfarin, direct oral anticoagulants) or antiplatelet agents (e.g., clopidogrel). For lesions less than 2 cm in size, I typically do not place prophylactic clips due to its lack of benefit and low bleeding risk, particularly if I used a cold snare polypectomy technique. In a recent systematic review and meta-analysis, Spadaccini et al showed there was no difference in post-polypectomy bleeding rates with or without prophylactic clip placement after resection of lesions less than 2 cm in size7. For lesions 2 cm in size or greater in the right colon, I routinely place prophylactic clips (e.g., Boston Scientific Resolution 360 Clip, MicroTech SureClip, Cook Instinct Endoscopic Clip) for prevention of post-EMR bleeding because of its thinner walls and higher bleeding risk2. However, as seen in this study and others, very large lesions (i.e., > 4 cm) may not be amenable for complete closure with prophylactic clips3-6. In these instances, I will coagulate all visible vessels with a coagulation grasper or with snare tip soft coagulation depending on the vessel size, and place clips at sites of potential deep mural injuries. Lastly, for patients with conditions that require prompt resumption of anticoagulation or antiplatelet agents, I routinely place prophylactic clips to decrease the risk of post-EMR bleeding, which has been shown to be cost-effective8.
For Future Research
More research is needed on effective closure methods for lesions greater than 4 cm, and lesions in the left colon removed by electrocautery.
Conflicts of Interest
Dr. Lee reports no conflicts of interest related to this study.
REFERENCES
- Kothari ST, Huang RJ, Shaukat A, et al. ASGE Standards of Practice Committee Chair. ASGE review of adverse events in colonoscopy. Gastrointest Endosc. 2019; 90(6):863-876.
- Metz AJ, Bourke MJ, Moss A, et al. Factors that predict bleeding following endoscopic mucosal resection of large colonic lesions. Endoscopy 2011; 43:506-11.
- Gupta S, Sidhu M, Shahidi N, et al. Effect of prophylactic endoscopic clip placement on clinically significant post-endoscopic mucosal resection bleeding in the right colon: a single-centre, randomised controlled trial. Lancet Gastroenterol Hepatol 2022; 7(2):152-160.
- Pohl H, Grimm IS, Moyer MT, et al. Clip Closure Prevents Bleeding After Endoscopic Resection of Large Colon Polyps in a Randomized Trial. Gastroenterology 2019; 157(4):977-984.
- Albéniz E, Álvarez MA, Espinós JC, et al. Clip Closure After Resection of Large Colorectal Lesions With Substantial Risk of Bleeding. Gastroenterology 2019; 157(5):1213-1221.
- Feagins LA, Smith AD, Kim D, et al. Efficacy of Prophylactic Hemoclips in Prevention of Delayed Post-Polypectomy Bleeding in Patients With Large Colonic Polyps. Gastroenterology 2019; 157(4):967-976.
- Spadaccini M, Albéniz E, Pohl H, et al. Prophylactic Clipping After Colorectal Endoscopic Resection Prevents Bleeding of Large, Proximal Polyps: Meta-analysis of Randomized Trials. Gastroenterology 2020; 159(1):148-158.
- Parikh ND, Zanocco K, Keswani RN, Gawron AJ. A cost-efficacy decision analysis of prophylactic clip placement after endoscopic removal of large polyps. Clin Gastroenterol Hepatol 2013; 11(10):1319-1324.