Screening Colonoscopy in the Elderly Population—Is Less Better?

Philip N. Okafor, MD, MPH
Senior Associate Consultant, Department of Gastroenterology, Mayo Clinic, Jacksonville, Florida
This summary reviews El Halabi J, Burke C, Hariri E, et al. Frequency of use and outcomes in individuals older than 75 years. JAMA Intern Med 2023; 183:519-19.
Correspondence to Philip N. Okafor, MD, MPH, Associate Editor. Email: EBGI@gi.org
Access the article through PubMed
STRUCTURED ABSTRACT
Question: When performing screening colonoscopy in individuals >75 years old, what is the frequency that life expectancy is <10 years and frequency of adverse events within 10-days of colonoscopy?
Design: This was a retrospective cross-sectional study using screening colonoscopy data between January 2009 and January 2022.
Setting: Cleveland Clinic in Ohio and Florida.
Participants: Asymptomatic individuals >75 years old who underwent colonoscopy for indication of screening. Patients with incomplete colonoscopy data, history of inflammatory bowel disease or colorectal cancer (CRC), or history of colonoscopy within past 5 years were excluded.
Intervention/Exposure: Screening colonoscopy complete to the cecum with an adequate bowel preparation.
Outcomes: The primary outcome was percentage of screening colonoscopies performed in individuals with <10 years life expectancy. Secondary outcomes were frequency of adverse events, defined as emergency visit or hospital admission, within 10-days of colonoscopy, and colonoscopy findings defined as normal, non-advanced polyps only (adenoma/hyperplastic polyp <10 mm) only, or advanced neoplasia (any adenoma >1 cm, villous adenoma, serrated adenoma, or CRC).
Data Analysis: Procedure details, colonoscopy and pathology findings were extracted using an internally validated natural language processing algorithm. Comorbidity-adjusted life expectancy at time of colonoscopy was estimated based on patients’ age and comorbidities from the Charlson comorbidity index using a standardized tool. Chart review was performed for each identified adverse event to assess likelihood of association between colonoscopy and adverse event using American Society for Gastrointestinal Endoscopy methodology.
Funding: None.
Results: In the cohort of 7,067 individuals undergoing screening colonoscopy, demographic data included 56% women, 77% White, and median age as 78 (interquartile range: 77-79) with 81.7% (n=5,775) between 76-80 years old, 14.4% (n=1,021) between 81-85 years old, and 3.8% (n=271) over 85 years old. The percentage of colonoscopies performed in individuals with life expectancy <10 years was 30% in the 76–80 year old cohort, 71% in the 81-85 year old cohort, and 100% in the >85 year old cohort (Table 1). Adverse event rate (hospitalization or emergency visit) was 13.6 per 1,000 patients, and individuals with life expectancy <10 years had approximately double the rate of adverse events as individuals with life expectancy >10 years. Prevalence of advanced neoplasia was 5.4% in 76–80 year olds, 6.2% in 81–85 year olds, and 9.5% in >85 year olds.
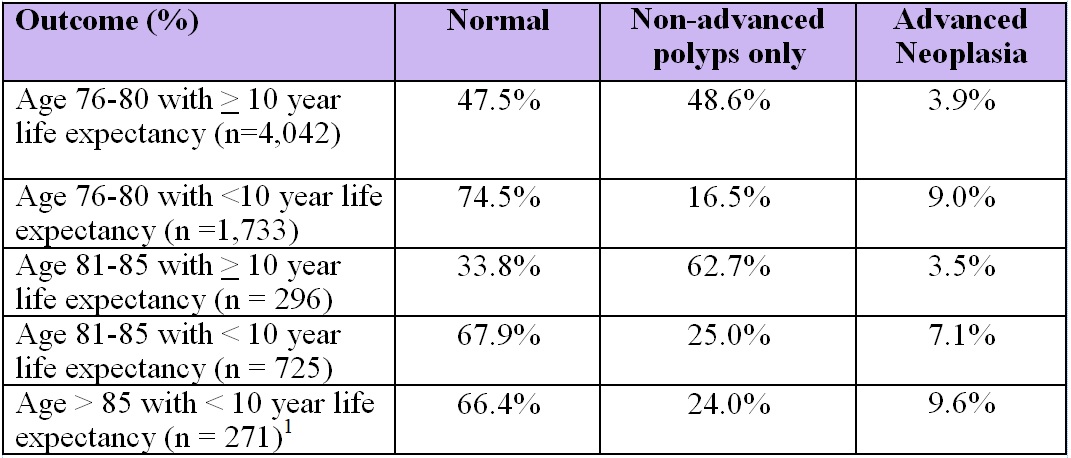
Table 1. Prevalence of advanced neoplasia, stratified by life expectancy < or > years.
1No patients >85-years old had a comorbidity-adjusted life expectancy of >10 years.
COMMENTARY
Why Is This Important?
Care that has a greater potential for harm than benefit is increasingly recognized in the United States and forms the basis of the American Board of Internal Medicine’s “Choosing Wisely” campaign1. Overtreatment occurs when there is little evidence of a clinically meaningful net benefit from an intervention. As it pertains to CRC screening, the 2021 United States Preventative Services Task Force recommendations for CRC screening in patients older than age 75 years come with a Grade C recommendation. This means that the selective recommendation of colonoscopies to individuals is based on professional judgment and patient preferences. Inadvertently, this may lead to indication creep which occurs when providers apply recommendations that may be appropriate for high-risk patients to all their patients2. Overscreening for CRC in patients older than 75 years is associated with physical and financial costs while often providing little benefit. This study by El Halabi et al provides supporting evidence of the low benefit and higher risk associated with most screening colonoscopies in patients older than 75 years, in a single health system in the United States.
Key Study Findings
They also observed a higher adverse event rate at 10 days which increased with age, especially among patients older than 85 years, suggesting that the risk of screening this group of patients was much higher than any derived benefit.
Caution
One limitation of this study is that it comes from a single health system which may limit secondary generalizability. In addition, in spite of the reports of lower advanced adenoma rates in their cohort, the study does not include data on colon polyp surveillance. It also does not compare outcomes between patients undergoing their first screening colonscopy vs those with a previous negative screening colonoscopy. The latter point is important to highlight as some studies have shown that colonoscopies in 76–80 year-olds do seem to reduce mortality due to CRC and the incidence of CRC, but only in patients who are “healthy,” meaning no prior myocardial infarction/stroke or no combination of diabetes, hypertension, elevated cholesterol, or coronary artery disease. The benefit was highest if no screening colonoscopies had been done prior to age 75.3
My Practice
The bulk of screening colonsocopies in my institution come from open access referrals. As a result, I see septuagenarians and octogenarians with significant comobididites still being referred for screening colonsocopies. To limit this, I try to document in the endoscopy report when further screening is not recommended, especially in patients 75 years and older, particularly if they have a high comorbidity burden. It is important to highlight: (1) the importance of estimating a patient’s life expectancy when making the decision to recommend screening colonoscopy in patients >75 years, and (2) the availability of online tools that allow a quick estimation of life expectancy that can be used in the decision-making process, including but not limited to ePrognosis.
For Future Research
Calderwood et al showed that up to 58% of older adults with less than 5-year life expectancy were recommended to return for future surveillance colonscopy4. This highlights that patient selection is the most important factor when recommending screening or surveillance colonoscopies in older adults. In addition, per the 2022 US Multi-Society Task Force recommendations, individuals with no prior screening colonoscopy who are 76-84 years and have a life expectancy of 5-10 years may be appropriate for offering screening colonoscopy based on patients’ preferences5. As such, intervention studies that assess the impact of provider education tools for estimating patient comorbidity burden and subsequent life expectancy on the decision to recommend screening colonoscopy in patients >75 years are needed to help reduce overscreening.
Conflict of Interest
Dr. Okafor reports no potential conflicts of interest.
@jessica_halabi
@burkegastrodoc
@majedrizkmd
REFERENCES
- American Board of Internal Medicine. Choosing Wisely: An Initiative of the ABIM Foundation. Accessed June 6, 2023. Available from: www.choosingwisely.org.
- Herzstein J, Ebell M. Improving quality by doing less: overtreatment. Am Fam Physician 2015; 91(5): 289-91.
- Lee JK. Screening colonoscopy decreases colorectal cancer incidence and colorectal-cancer related mortality in patients >75 years old…as long as they are healthy! Evidence-Based GI. Oct 22, 2021. https://gi.org/journals-publications/ebgi/lee_october2021/.
- Calderwood AH, Tosteson TD, Qang Q, et al., Association of life expectancy with surveillance colonoscopy findings and follow-up recommendations in older adults. JAMA Intern Med 2023; 183(5): 426-434.
- Patel SG, Folasade MP, Anderson J, et al. Updates on age to start and stop colorectal cancer screening: Recommendations from the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol 2022; 117;(1): 57-69.